I need help to stay consistent and schedule my goal and print it in the kitchen to see it, as if my life depends on it. My family needs to support my diet goals. My family doesn't know my goals and aren't reading my food diary and I don't have the support I need.
I don't know what foods to eat. We need to make an updated diet plan based on my notes from this diary for January and stick to it.
Now I may need to juice fast again and start all over. Very frustrating.
diet plan with 1 cup meat (less meat)

no meat, 30 almonds

Supplements on sibo diet
Supplements on sibo diet
B vitamin
Vit d
More calcium
SIBO MEAL PLAN/SCHEDULE:
"ELEMENTAL/SAFE DIET FOR 2 WEEKS"
-Turkey every 2nd day.
-Herbal antibiotics for 4 weeks (peppermint/cinnamon, need to find an alternative one: chinese bitters or my herbal drink.)
HERBAL ANTIBIOTICS TO ROTATE:
cinnamon (causes constipation but works well)
peppermint (daily use)
cayenne pepper (alternate with cinnamon?)
rose hips (tea?)
italian herbs (sage, oregano, etc)
LESSONS FROM THE NOTES BELOW:
"ELEMENTAL/SAFE DIET FOR 2 WEEKS"
-Turkey every 2nd day.
-Herbal antibiotics for 4 weeks (peppermint/cinnamon, need to find an alternative one: chinese bitters or my herbal drink.)
HERBAL ANTIBIOTICS TO ROTATE:
cinnamon (causes constipation but works well)
peppermint (daily use)
cayenne pepper (alternate with cinnamon?)
rose hips (tea?)
italian herbs (sage, oregano, etc)
Natural Cures: Peppermint oil (enterically coated) has been studied and found to reduce the number of microbes in the small intestine. Oregano, garlic, goldenseal, and cinnamon may also help to control bacterial levels within the small intestine, to reduce symptoms of SIBO: http://earthclinic.com/CURES/sibo.html
LESSONS FROM THE NOTES BELOW:
-create sibo meal plan for today and check if enough nutrients. Include cinnamon, ginger and sibo treatment. Take potassium mag. Test 1 cup meat today.
-schedule diet with water and supp (vit d)
-FIND HERBALIST to help me with dosage of these herbs (cloves, etc)
-reduce meat protein at first, OR take more bitters with every protein meal (lots of ginger + herbal drink)
-take cinnamon/peppermint 3x at every meal
-research glutamine
-research if its worth doing a test ($115 for breath test, OAT unknown)
-review previous OAT test
-review AC response https://mail.google.com/mail/u/0/#search/oat+test/13ed925f3028b79b
-review calcium issue and low carb (should i return to low carb? if so, what supp should i take? i don't want to lower my calcium and cause other problems like the previous ones i had - including teeth!)
-dr philip: test vitamin d, over 60 is good, for bone problem.
-make a list of most important supps to try and ask my health team opinion:
-make a list of most important supps to try and ask my health team opinion:
Next to try:
multivitamin
Vit d (low reaction)
ALA
Chinese bitters (for digestion) unsure.
Milk thistle tincture (maybe low)
Siberian Eleuthero
Frankinscence (maybe unsure)
SIBO
http://www.townsendletter.com/FebMarch2013/ibs0213_2.html
http://chriskresser.com/rhr-testing-for-sibo-graves-disease-and-all-about-anemia
PLAN LOW FERMENTABLE FOODS;
Three Part Strategy In order to successfully treat IBS, the destructive cycle of malabsorption, bacterial overgrowth, and inflammation must • First, address any underlying condition( s) that promote( s) SIBO on a case-by-case basis (the subject of the rest of this chapter.
Potential causes of SIBO (you likely suffer from one or more of these if you have IBS or heartburn) can be grouped into five categories:
- Motility issues
- Antibiotic use
- Gastric (stomach) acid reduction
- Immune impairment
- Carbohydrate malabsorption
constipation-predominant IBS (IBS-C) is associated with microbes that produce methane gas.[ 85 ],[ 86]
Problems that can lead to alteration in motility include: • Structural defects of the intestine • Aging • Intestinal infections • Narrowing of the intestine due to scarring from Crohn's Disease or scleroderma • Surgical alteration of the intestine • Damage to the vagus nerve • Hypothyroidism.
Damage to the vagus nerve from years of high blood sugar in type I and type II diabetes can result in prolonged gut transit times because th the vagus nerve normally signals the muscles surrounding the intestine to contract . Similarly , intestinal motor dysfunction associated with hypothyroidism has been linked to SIBO.[ 87
BAD PROBIOTICS:
Some brands of probiotics are associated with bloating. Bloating can be caused by including bacterial strains that (unlike Lactobacillus acidophilis, a homolactic fermenter which produces no gas) are capable of producing gas from carbohydrates. These strains include: Lactobacillus brevis, Lactobacillus casei, Streptococcus thermophilus and probiotic yeast strains. (My probiotic contains casei, and brevis!)
TESTING FOR SIBO
One, and the most common one is a breath test, where you drink a solution that contains some simple sugars, which can be fermented by small intestine bacteria. And then you blow into a little tube that’s attached to a balloon or a bag, and then you send that bag to the lab, and the lab tests it for certain gases that are produced by certain kinds of bacteria. And if the levels of the gases are high, then that indicates you have an overgrowth of bacteria in the small intestine. So that’s one way of testing for it. Another way of testing for it is a urine organic acids test, and these are offered by labs like Metametrix and Genova Diagnostics, who just bought Metametrix actually last week, so they’re gonna be merging together. And organic acids are byproducts of bacterial metabolism. So certain types of organic acids, if they’re elevated in the urine, can indicate an overgrowth of bacteria in the gut and also an overgrowth of fungi. So D-arabinitol is an organic acid that’s produced in fungal metabolism, and so if you have an overgrowth of D-arabinitol in the urine, then that can indicate a yeast overgrowth.
So those are the two main tests. I tend to use the organic acids test more, and that’s partly because it has a number of markers that I find to be useful, and so I just can kill several birds with one stone, and I tend to order that more, but the breath test is also good. One lab that’s pretty well known for the breath test is Metabolic Solutions, and it’s pretty affordable. It’s like a hundred bucks,
And I see this a lot on people who start a paleo diet coming from a diet with less animal protein. We’ve talked about tons of times on the show. Stomach acid, as you all know by now, is crucial to breaking down protein, particularly animal protein, and if you don’t have enough stomach acid, the protein can putrefy in the stomach. And I haven’t seen any research on this from a conventional medical perspective, but certainly anyone who is familiar with Chinese medicine will know that they put a lot of stock into the appearance of the tongue, and a thick coating on the tongue is definitely an indicator of digestive disharmony. And I don’t really know how to explain that with precision from a Western medical paradigm perspective, but I certainly have seen it to be, you know — In nearly everyone who has a digestive issue, there tends to be a coat on the tongue. So that’s my guess: low stomach acid. It could also be small bowel bacterial overgrowth, and we talked earlier about how to get tested for that. The easiest thing to do to test out the stomach acid hypothesis would be to just take some hydrochloric acid, that betaine HCl protocol. We’ll put a link in the show notes to the post on my website where I discuss the protocol in detail and go through it step by step. And if that doesn’t work, I would probably get tested for SIBO. Or if you do the organic acids test, that will test for both SIBO and a fungal overgrowth, which would probably be an even better idea.
OAT TEST interpretation;
http://www.metametrix.com/files/test-menu/interpretive-guides/Organix-IG.pdf
Glutamine, 10–20 gm daily, digestive aids (betaine,
enzymes, bile) and free-form amino acids help to normalize
gut permeability
These compounds may reflect intestinal overgrowth,
usually accompanied by microbial hyperpermeability.
Take appropriate steps to ensure favorable gut microflora
population.
BREATH TEST:
http://www.metsol.com/sibo-breath-test/preparation
$115
Bitters
Another way to stimulate acid production in the stomach is by taking bitter herbs. “Bitters” have been used in traditional cultures for thousands of years to stimulate and improve digestion. More recently, studies have confirmed the ability of bitters to increase the flow of digestive juices, including HCL, bile, pepsin, gastrin and pancreatic enzymes. 1
Unsurprisingly, there aren’t many clinical studies evaluating the therapeutic potential of unpatentable and therefore unprofitable bitters. However, in one uncontrolled study in Germany, where a high percentage of doctors prescribe herbal medicine, gentian root capsules provided dramatic relief of GI symptoms in 205 patients.
The following is a list of bitter herbs commonly used in Western and Chinese herbology:
- Barberry bark
- Caraway
- Dandelion
- Fennel
- Gentian root
- Ginger
- Globe artichoke
- Goldenseal root
- Hops
- Milk thistle
- Peppermint
- Wormwood
- Yellow dock
Bitters are normally taken in very small doses – just enough to evoke a strong taste of bitterness. Kerry Bone, a respected Western herbalist, suggests 5 to 10 drops of a 1:5 tincture of the above herbs taken in 20 mL of water.
Diet
A lower-carbohydrate diet is used in combination with a prokinetic to discourage a return of overgrowth of bacteria by limiting the food that they thrive on. Once the overgrowth is gone and small intestine damage has healed, the diet can be expanded beyond the strictness of the SCD and GAPS diets. The time frame for this is uncertain. To our knowledge, only one study has examined the rate of healing post SIBO, which found that intestinal permeability normalized four weeks after successful SIBO eradication in 75% of patients.37 While this report is very encouraging, it may or may not reflect the other repair needed post SIBO. Therefore we currently suggest continuing a SIBO diet for three months post successful eradication. At this point, the Cedars-Sinai Diet, FODMAP Diet, or a similar lower-carb diet may be adopted long term, as the patient tolerates.28,61These diets allow more carbohydrates in the form of grains, gluten-free grains, sugar, and soy, though they still limit overall carbohydrate amounts.
Spacing meals 4 to 5 hours apart, with nothing ingested but water, allows migrating motor complex (MMC) to occur.28 We have found this to be very helpful clinically. If a low-carb SIBO diet does not correct hypoglycemia, this strategy will need to be altered to allow for more frequent meals.
In our practices we have found that the following circumstances increase the chances for an unsatisfactory patient outcome:
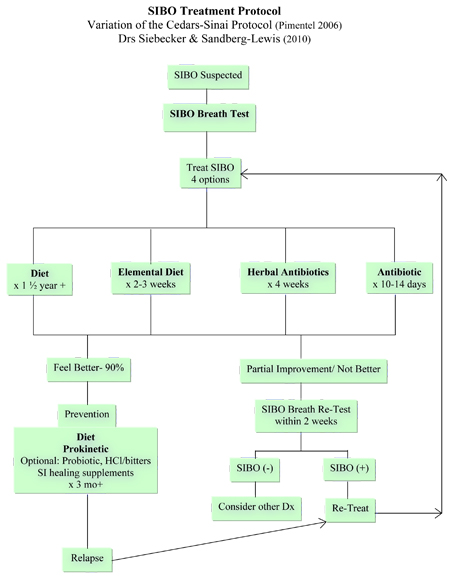
• Failure to continue treatment courses until SIBO is eradicated (negative breath test or patient ≥90% better). This crucial process of successive treatment is indicated by the long go-back arrow on the right side of our algorithm (Figure 3).
• Failure to use double antibiotic therapy for methane producers. Methanogenic bacteria need different antibiotic treatment than hydrogen-producing bacteria.
• Failure to utilize breath testing to identify if the patient has SIBO, the type of gas he/she produces, and the overall level of gas. This information is necessary for diagnosis, treatment choice, duration, and prognosis.
• Failure to use a prokinetic immediately following treatment. Prokinetics along with diet are needed to prevent relapse of this commonly recurring condition.
• Failure to use a low-carb preventative diet following treatment. Diet along with prokinetics are needed to prevent relapse of this commonly recurring condition.
• Failure to tailor diet to individual tolerances with personal experimentation. No fixed diet can predict an individual's complex bacterial, digestive, absorptive, immunological, and genetic circumstances; therefore customizing is necessary.
• Failure to identify underlying causative conditions. A recent report found the following conditions led to a poor response to antibiotics: anatomical abnormalities, chronic narcotic use, Addison's disease, scleroderma, colonic inertia, inflammatory bowel disease, and NSAID-induced intestinal ulceration.69
Treatment of SIBO
In 2006, Pimentel shared his treatment algorithm for IBS with SIBO which included the use of either antibiotics, elemental diet or both.28 Our approach offers two additional options: diet and herbal antibiotics (Figure 3).
In 2006, Pimentel shared his treatment algorithm for IBS with SIBO which included the use of either antibiotics, elemental diet or both.28 Our approach offers two additional options: diet and herbal antibiotics (Figure 3).
Figure 3
Diet
We advise diet (Specific Carbohydrate Diet or Gut and Psychology Syndrome Diet) for all SIBO patients.42,43 Since bacteria use carbohydrates as their energy source and ferment them to gas, a low-carbohydrate diet can directly reduce symptoms by decreasing the amount of gas produced.44Reducing carbohydrates may also reduce the overall bacterial load as the food supply shrinks, though formal studies to validate this are lacking. These diets decrease polysaccharides, oligosaccharides, and disaccharides by eliminating all grains, starchy vegetables, lactose, sweeteners other than honey, and in the beginning, beans. Many patients experience a rapid and significant decrease in symptoms after starting a SIBO diet. The Specific Carbohydrate Diet (SCD) has been reported to have an 84% success rate for inflammatory bowel disease, a condition commonly associated with SIBO.45,46
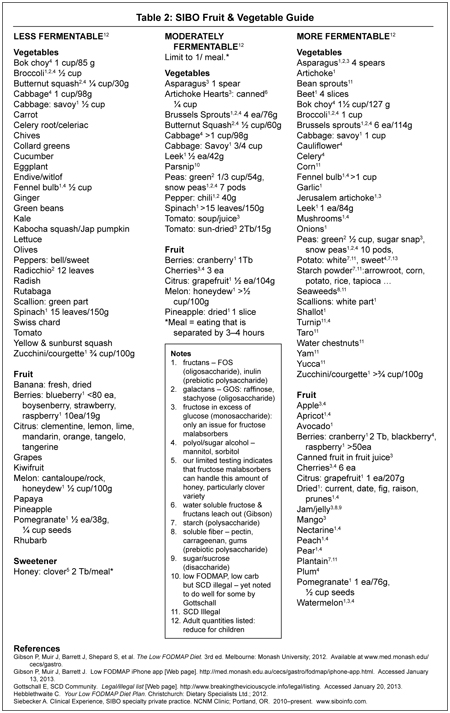
Diet alone has proven successful for infants and children, but for adults one or more of the other three treatment options are often needed to reduce bacteria quickly, particularly in cases in which diet needs to be very restricted to obtain symptomatic relief. Additionally, any diet will always need to be customized to the individual by trial and error over time. That being said, following a diet prescription offers a place to start. We have found that using the SCD or Gut and Psychology Syndrome Diet (GAPS) as the core diet (Table 1), with the incorporation of the fruit and vegetable recommendations from the Low FODMAP Diet (Table 2), is an effective approach. The Low FODMAP Diet is an IBS treatment diet that has investigated the fermentable levels of carbohydrate foods (fruits, vegetables, and grains) and has a success rate of 76%.47 The FODMAP Diet is not specifically designed for SIBO and therefore does not eliminate polysaccharide and disaccharide sources such as grains, starch, starchy vegetables, and sucrose. Eliminating these poly- and disaccharides is essential in SIBO because SIBO creates a situation in which these normally well-absorbed carbohydrates, foods that usually go to feed the host, can now feed bacteria inappropriately located in the small intestine, creating symptoms and worsening the problem (Figure 1).
We advise diet (Specific Carbohydrate Diet or Gut and Psychology Syndrome Diet) for all SIBO patients.42,43 Since bacteria use carbohydrates as their energy source and ferment them to gas, a low-carbohydrate diet can directly reduce symptoms by decreasing the amount of gas produced.44Reducing carbohydrates may also reduce the overall bacterial load as the food supply shrinks, though formal studies to validate this are lacking. These diets decrease polysaccharides, oligosaccharides, and disaccharides by eliminating all grains, starchy vegetables, lactose, sweeteners other than honey, and in the beginning, beans. Many patients experience a rapid and significant decrease in symptoms after starting a SIBO diet. The Specific Carbohydrate Diet (SCD) has been reported to have an 84% success rate for inflammatory bowel disease, a condition commonly associated with SIBO.45,46
Diet alone has proven successful for infants and children, but for adults one or more of the other three treatment options are often needed to reduce bacteria quickly, particularly in cases in which diet needs to be very restricted to obtain symptomatic relief. Additionally, any diet will always need to be customized to the individual by trial and error over time. That being said, following a diet prescription offers a place to start. We have found that using the SCD or Gut and Psychology Syndrome Diet (GAPS) as the core diet (Table 1), with the incorporation of the fruit and vegetable recommendations from the Low FODMAP Diet (Table 2), is an effective approach. The Low FODMAP Diet is an IBS treatment diet that has investigated the fermentable levels of carbohydrate foods (fruits, vegetables, and grains) and has a success rate of 76%.47 The FODMAP Diet is not specifically designed for SIBO and therefore does not eliminate polysaccharide and disaccharide sources such as grains, starch, starchy vegetables, and sucrose. Eliminating these poly- and disaccharides is essential in SIBO because SIBO creates a situation in which these normally well-absorbed carbohydrates, foods that usually go to feed the host, can now feed bacteria inappropriately located in the small intestine, creating symptoms and worsening the problem (Figure 1).
Table 1
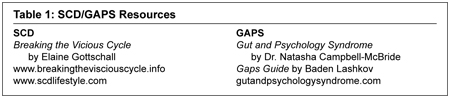
Table 2
Low-carbohydrate diets are weight-loss diets. Particular attention must be paid to those who are low weight or underweight. If a low-carb SIBO diet is causing too much weight loss, this dietary strategy will need to be altered to allow for more carbohydrates. In these circumstances, one or more of the other three treatment options should be considered along with white rice, glucose, and other carbohydrate sources.
Diet is also essential for prevention, post SIBO treatment.
Elemental Diet
An elemental diet can be used in place of antibiotics or herbal antibiotics to rapidly decrease bacteria. Elemental diets are powdered predigested nutrients that are mixed with water and used in hospitals for various gastrointestinal disorders to give digestion a rest. The concept behind this treatment for SIBO is that the nutrients will be absorbed before having a chance to feed the bacteria, thus feeding the person but starving the bacteria. It is used in place of all meals, for 2 to 3 weeks, and has a success rate of 80% to 85%.48 Elemental diets are not protein powders or cleansing/detox formulas. They are available over the counter and are not covered by insurance, which can make this treatment course costly.
An elemental diet can be used in place of antibiotics or herbal antibiotics to rapidly decrease bacteria. Elemental diets are powdered predigested nutrients that are mixed with water and used in hospitals for various gastrointestinal disorders to give digestion a rest. The concept behind this treatment for SIBO is that the nutrients will be absorbed before having a chance to feed the bacteria, thus feeding the person but starving the bacteria. It is used in place of all meals, for 2 to 3 weeks, and has a success rate of 80% to 85%.48 Elemental diets are not protein powders or cleansing/detox formulas. They are available over the counter and are not covered by insurance, which can make this treatment course costly.
Antibiotics
The most studied and successful antibiotic for SIBO is rifaximin. It has a broad spectrum of activity and is nonabsorbable. Its nonabsorbability allows it to stay in the intestine, acting locally and it is therefore less likely to cause systemic side effects common to standard absorbable antibiotics.49Rifaximin has up to a 91% success rate and is given at 550 mg t.i.d × 14 days.50,51 Additionally, rifaximin has several unique benefits: it does not cause yeast overgrowth, it decreases antibiotic resistance in bacteria by reducing plasmids, antibiotic resistance does not develop to it, making it effective for retreatments, and it is anti-inflammatory, decreasing intestinal inflammatory cytokines and inhibiting NF-kb via the PXR gene.52–54 Rifaximin is best used for SIBO when hydrogen is present, but when methane gas is present, double therapy of rifaximin plus neomycin (500 mg b.i.d. × 14 days) is more effective.55 Many gastroenterologists use metronidazole (250 mg t.i.d. × 14 days) as an alternative to neomycin (unpublished). Since different antibiotic regimens are recommended based on the gas type, breath testing is necessitated when considering this treatment.
The most studied and successful antibiotic for SIBO is rifaximin. It has a broad spectrum of activity and is nonabsorbable. Its nonabsorbability allows it to stay in the intestine, acting locally and it is therefore less likely to cause systemic side effects common to standard absorbable antibiotics.49Rifaximin has up to a 91% success rate and is given at 550 mg t.i.d × 14 days.50,51 Additionally, rifaximin has several unique benefits: it does not cause yeast overgrowth, it decreases antibiotic resistance in bacteria by reducing plasmids, antibiotic resistance does not develop to it, making it effective for retreatments, and it is anti-inflammatory, decreasing intestinal inflammatory cytokines and inhibiting NF-kb via the PXR gene.52–54 Rifaximin is best used for SIBO when hydrogen is present, but when methane gas is present, double therapy of rifaximin plus neomycin (500 mg b.i.d. × 14 days) is more effective.55 Many gastroenterologists use metronidazole (250 mg t.i.d. × 14 days) as an alternative to neomycin (unpublished). Since different antibiotic regimens are recommended based on the gas type, breath testing is necessitated when considering this treatment.
Herbal Antibiotics
While there has only been one published report of herbal antibiotics in the treatment of SIBO, our experience is that they have similar effectiveness to antibiotics.56 We have used the following botanicals: Allium sativum, Hydrastis canadensis, and other berberine-containing herbs, Origanum vulgare, cinnamon, and Azadirachta indica. We have used these as both single agents and in various combinations at dosages that are at the upper end of label suggestions × 30 days. Specific single dosages we have used include allicin extract of garlic: 450 mg b.i.d.–t.i.d., goldenseal/berberine: 5g q.d. in split dosage, emulsified oregano: 100 mg b.i.d., and neem: 300 mg t.i.d. Our breath testing has validated the need for the longer treatment period of 30 days for herbal antibiotics compared with 14 days for antibiotics. We have also observed with this method prolonged die-off reactions, which can last for the duration of treatment course. Studies on herbal antibiotics for SIBO are needed, particularly to identify botanicals effective in reducing methane.
While there has only been one published report of herbal antibiotics in the treatment of SIBO, our experience is that they have similar effectiveness to antibiotics.56 We have used the following botanicals: Allium sativum, Hydrastis canadensis, and other berberine-containing herbs, Origanum vulgare, cinnamon, and Azadirachta indica. We have used these as both single agents and in various combinations at dosages that are at the upper end of label suggestions × 30 days. Specific single dosages we have used include allicin extract of garlic: 450 mg b.i.d.–t.i.d., goldenseal/berberine: 5g q.d. in split dosage, emulsified oregano: 100 mg b.i.d., and neem: 300 mg t.i.d. Our breath testing has validated the need for the longer treatment period of 30 days for herbal antibiotics compared with 14 days for antibiotics. We have also observed with this method prolonged die-off reactions, which can last for the duration of treatment course. Studies on herbal antibiotics for SIBO are needed, particularly to identify botanicals effective in reducing methane.
Prevention of SIBO
SIBO is a disease that relapses because eradication itself does not always correct the underlying cause.57,58 Pimentel's 2006 treatment algorithm includes 2 essential preventions: diet and a prokinetic (motility agent). Our approach offers 3 optional additions: hydrochloric acid, probiotics, and brush border healing supplements (Figure 3).
SIBO is a disease that relapses because eradication itself does not always correct the underlying cause.57,58 Pimentel's 2006 treatment algorithm includes 2 essential preventions: diet and a prokinetic (motility agent). Our approach offers 3 optional additions: hydrochloric acid, probiotics, and brush border healing supplements (Figure 3).
Prokinetic
A key underlying cause of SIBO is thought to be deficiency of the migrating motor complex (MMC), which moves bacteria down into the large intestine during fasting at night and between meals.59 Prokinetics stimulate the MMC, symptomatically correcting this underlying cause. Prokinetics studied for SIBO include low-dose naltrexone 2.5 mg q.d., h.s., or b.i.d., low-dose erythromycin 50 mg h.s., and tegaserod 2–6 mg h.s.59,60 Tegaserod has a higher success rate for SIBO prevention versus erythromycin, but has been withdrawn from the US for safety reasons.59Prucalopride 1–4 mg h.s. is not yet available in the US but is a safer alternative to tegaserod.61 A trial removal of the prokinetic at ≥ 3 months is suggested but continued long-term use may be needed.28
No comments:
Post a Comment